Reframing DEE-SWAS for families
There is a gap between clinical language and what life with DEE-SWAS is like for my child and family in the conversations that matter most.
There is no clear, simple way to talk about DEE-SWAS with my children, families and friends, and the teachers, health, disability and community professionals in our life.
As a parent, I become the interpreter and translator when important information about my child’s rare epilepsy needs to be shared.
As a writer who has worked on reframing projects that deepen understanding of poverty and other complex problems, a clear, accurate communications toolkit to help me talk about DEE-SWAS is something that would help me immensely.
What is reframing?
Reframing is not just changing language. It involves systematically identifying how an issue (or condition) is understood across different groups and what the misunderstandings and unhelpful assumptions are. The next step is developing clear, consistent ways of explaining what is happening, why it matters, and what helps. For DEE-SWAS, this would mean drawing on lived experience, clinical knowledge and research to map the common narratives (for example, “it’s behavioural”, “they’re not trying”, or “they look fine”), and then testing alternative explanations that better reflect the underlying brain-based disruption to learning, language, fatigue and identity. It would involve developing and trialling messages, stories and practical communication tools with educators, allied health professionals, disability support workers, parents, children, clinicians and researchers, then refining them based on what improves understanding and response. The aim would be a shared, accessible way of talking about DEE-SWAS so that people are not working from fragmented or conflicting interpretations, but from a common understanding of the child’s experience. Similar structured approaches have been developed in areas like child and family mental health, but there is currently no equivalent for epilepsy that I know of. It could reduce blame, improve alignment across systems, and support more appropriate, informed responses to children with DEE-SWAS and other developmental and epileptic encephalopathies (DEEs) and their families.
Things don’t go as well when I don’t have the right words
I have experienced that how well I am able to talk about this rare syndrome heavily influences how my child’s needs and evolving sense of self are understood, and the support they can access to participate in everyday life.
A neurologist might talk about spike-and-wave (SWI) activity, but I am the one who has to convey it to my child in terms of why they often feel tired, frustrated and cloudy-headed. I am the one in the principal’s office explaining the impact on learning, attention and behaviour. I am trying to explain to grandparents why it’s not a naughty kid or bad parenting. And I am doing all of this while feeling scared, sad, overwhelmed and low in confidence that I’m doing it right. Right now, there is no consistent support to help bridge this gap.
I’m very tired and worried but I must adapt constantly to connect with my ‘audience’
I’m not only imparting information for the different people in my child’s life - I am adapting how I talk about it. In a medical setting, where my child is being treated for rare epilepsy, it’s the language of the medical model. But my child also has anxiety - a paediatrician’s domain. At the paediatrician’s clinic we speak in the recovery model. Then I’m talking to my child’s teacher at school, where they are perceived through an autism lens. In that setting, talking about the loss DEE-SWAS has brought is not always considered strength based or neuro-affirming. There is no consistent guidance on how to navigate this, and getting it wrong can affect how holistically my child is understood and supported.
Identity transition
The other part of this journey that has not been well recognised is the clear “before and after”. My child’s rare epilepsy emerged at age 7.
Before, they were living a typical kid’s life, with friendships, weekend sport and birthday parties, and full participation in learning. Digging up veges in the garden, joyfully chasing chickens and reading short novels. Over a period of months, changes emerged. Emergency medical care for clinical seizures began. In parallel, a dramatic cognitive shift unfolded. It was so subtle at first that only their teacher noticed, but the changes accelerated, bringing profound grief and fear to our family.
In less than a year, our typically developing child transitioned to being a child with significant disability, abruptly cut off from many of the experiences we had taken for granted. Their school, sport and playdates - all gone.
My child with DEE-SWAS will at times reflect on their embarrassment about some behaviours during the most difficult times, express self-blame and nostalgia for lost abilities, and uncertainty about where they belong among peers.
If this were an adult with dementia, far more would be done to support that transition for both the person and their family. In this case, strategies don’t exist, so very little is able to be done. In fact, the emotional and psychological toll of this identity shift, on our child and on our family, has never been explicitly acknowledged outside our household.
I’ve read that clinicians themselves can struggle with how to help families navigate hope and uncertainty. They need to be honest about difficult realities while still offering a form of hope that is meaningful, credible, and does not cause harm. How incredibly hard (1).
That makes me wonder whether part of what’s missing is a shared way of communicating. Something that helps bridge how clinicians, families, educators and others talk about these conditions. If even clinicians are navigating how to hold hope and uncertainty in words, it’s not surprising that families are left carrying this alone across every setting. A gentle, consistent communication framework could help. Not to simplify the reality, but to make it more understandable and more human across these important settings. For children with DEE-SWAS, this might also include developmentally appropriate ways of explaining their experiences, such as simple narratives or social stories, so they are not left trying to make sense of it without support.
I truly believe a communications framework for how we communicate about DEE-SWAS and other DEEs would help my child and family immensely. It could help ensure that children’s lived experience is consistently understood in all the most meaningful parts and by the most important people in their lives. In doing so, we create the possibility of care and support that is truly joined up, where children like mine are holistically understood and therefore more able to participate, belong and thrive.
A note on the social story
This is a simple social story I created using AI to help explain my child’s experience of DEE-SWAS. I haven’t shared it with them - it’s something I’m experimenting with. And I’m not sure it fully aligns with best practice in supporting children with disability.
I would welcome more research-informed guidance on how to talk with my child, their teachers and various specialists about DEE-SWAS in a way that protects their identity and voice and supports connection and participation.
- Melanie
1. Nevin, S.M., Beavis, E., Macintosh, R., Palmer, E.E., Sachdev, R., Le Marne, F.A., Bye, A.M. and Nunn, K. (2022), Hope in the uncertainties and certainty for parents of children with rare neurological disorders: Part 2 (of 3): Certainty. J Paediatr Child Health, 58: 1722-1725. https://doi.org/10.1111/jpc.16202
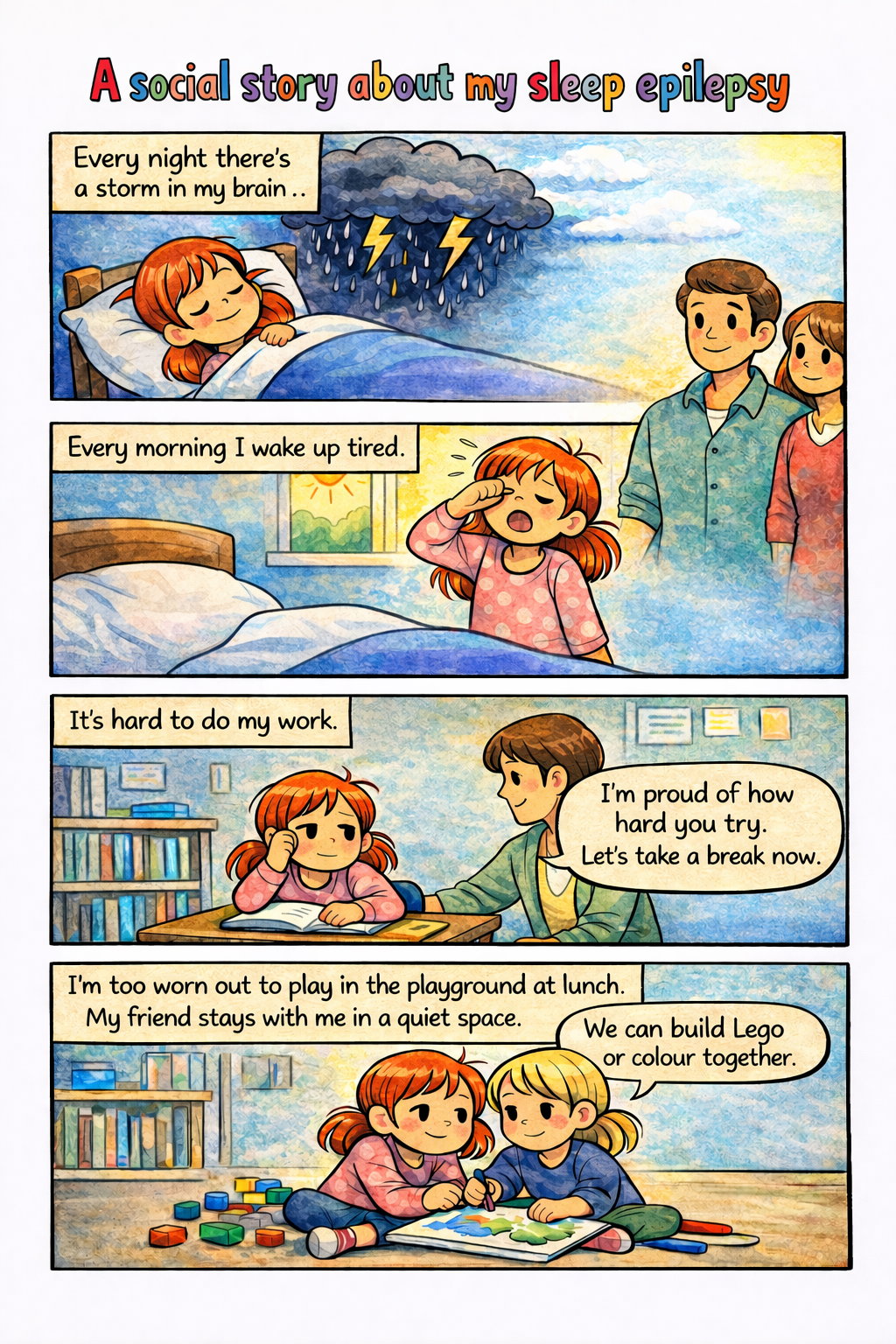
A (draft) social story I created. If I had a way to know I was on the right track with this, I could share it with my child to talk about why they feel tired at school and learning is hard. It could also help prepare them for the adjustments they will receive at school.